Samuel Edusa MD
The near tragedy during Monday Night Football - The Damar Hamlin Incident. Was It Commotio Cordis?
Collins A. Kwarteng MD, FACC | Jan 4, 2023
Originally published by Collins A. Kwarteng, MD, FACC. Reproduced here with the author's permission.

I am sure by now almost everyone in America and across the globe who was glued to his/her TV watching the MNF game between the Buffalo Bills and the Cincinnati Bengals, witnessed the surreal incident of the sudden collapse of a Buffalo Bills defensive player, Damar Hamlin. A lot has been said about what may have happened. As usual, there have been a lot of conspiracy theories as to what may have happened.
I was neither present at the scene nor have I had any inside information from the medical staff to have any first-hand knowledge to say what I am about to say. I am ONLY deducing from what I witnessed, as to what may have happened.
So it appears that he went in to tackle the Bengals tightened, #85, who lowered his head with his helmet making contact with Hamlin's chest. He seemed to get up briefly, then collapse and fall backward into a supine position and appear to immediately start some sort of a slight jerking movement.
The consensus from the medical community is that the impact is what caused that arrest. The fact is we don't know. But how does a blunt force trauma to the chest cause a cardiac arrest, which he is alleged to have suffered?
The phenomenon of acute cardiac arrest, caused by an acute blunt force trauma, is called COMMOTIO CORDIS.
It happens when there is a sudden blunt force to the chest as happened in this case, or during a head-on-collision in a motor vehicle accident where the chest hits the steering wheel; a baseball or a hockey puck to a specific location in the anterior chest wall, at an exact time of the heart's electrical cycle.
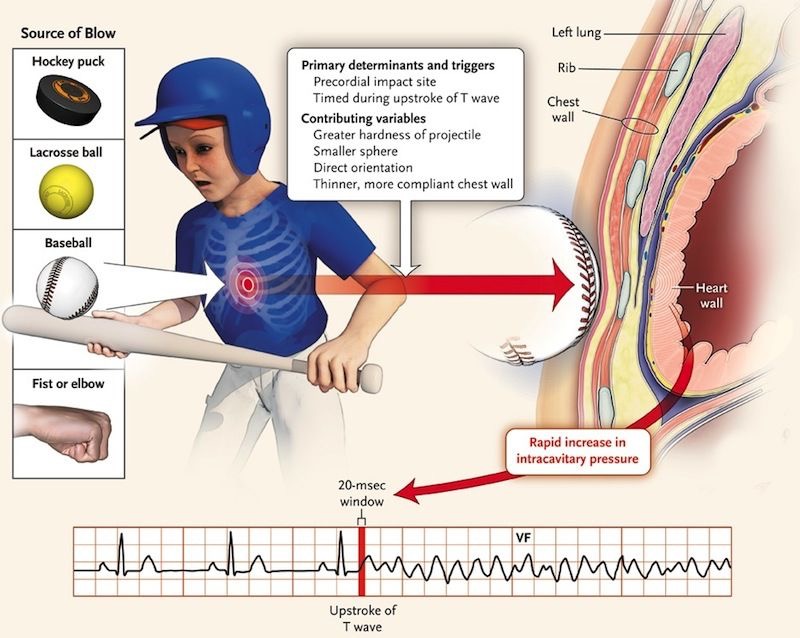
The force to the chest, in and of itself, DOES NOT cause this phenomenon, but it must be timed perfectly to happen during repolarization/resetting of the heart's electricity for commotio cordis to occur.
The heart's cycle, one cardiac cycle, starts from depolarization of the atrium, the p-wave, and ends with repolarization of the ventricle, the T-wave. See below.
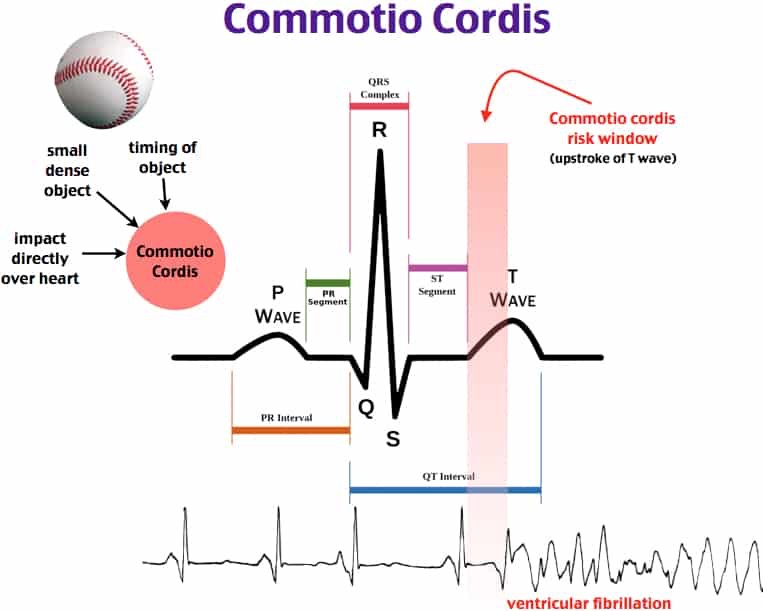
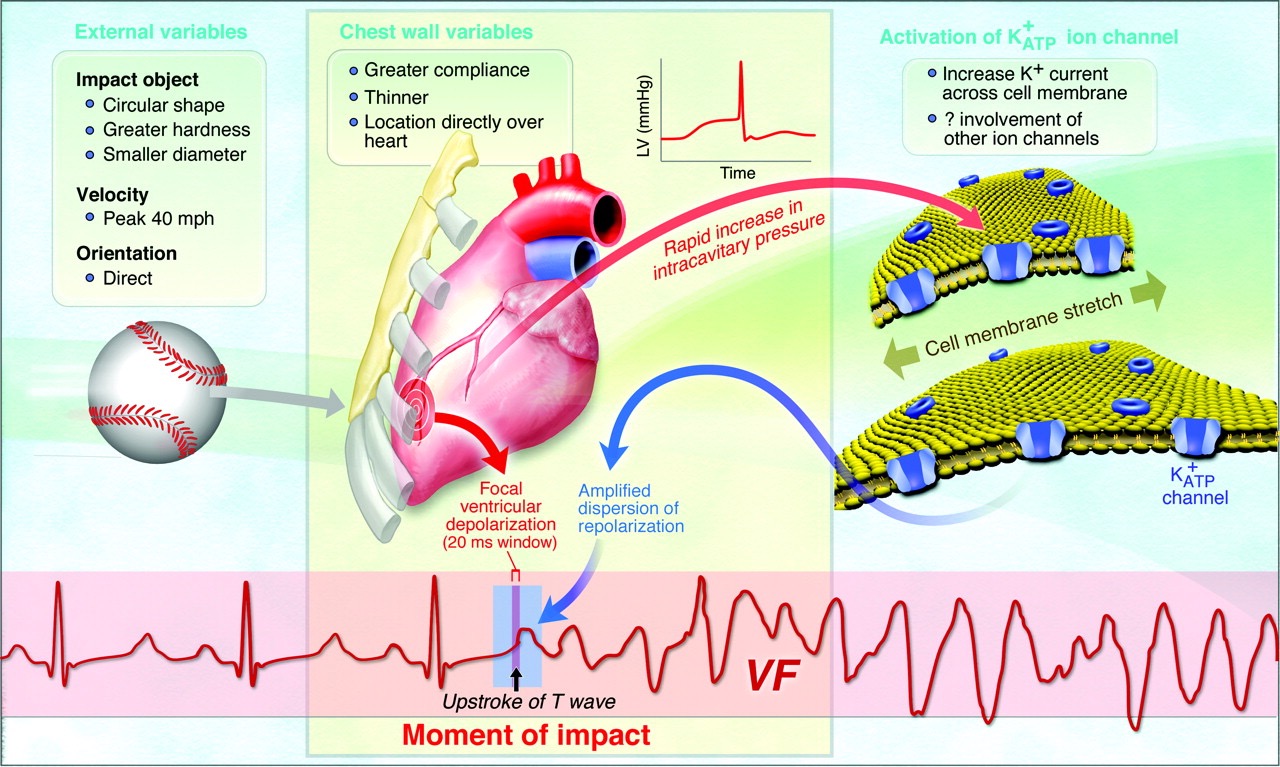
If the blunt-force trauma happens to occur just at the upstroke of the ventricular repolarization of the heart's electrical cycle (upstroke of the T-wave), with the right amount of force, at the right location and orientation of the vector of the force to the chest wall, then it can lead to a sudden malignant arrhythmia called ventricular fibrillation or V-fib, or in simple layman's terms, a sudden cardiac arrest! This perfectly timed blunt-force, impact-induced cardiac arrest is what's called COMMOTIO CORDIS!
The gold standard of management is to immediately identify that it has happened, confirm that there is a death spiral caused by v-fib, AND IMMEDIATELY SHOCK or defibrillate the heart. In other words, just Cranck up the AED AND SHOCK! Once the rhythm is confirmed to have been broken and converted back to normal rhythm (normal sinus rhythm) then you confirm to make sure that the rhythm you are seeing is associated with a palpable pulse. If there is no pulse, then and then only do you do chest compressions. The presence of a rhythm without a pulse is a PEA, or a Pulseless Electrical Activity, which would require continuous CPR while looking to identify reversible causes like acidosis, acute occlusive pulmonary embolism, electrolyte abnormalities, hypoglycemia, etc.
Sometimes, the sudden cardiac arrhythmia can occur spontaneously without any external provocation. That tends to happen in inherited cardiac electrical channel problems or channelopathies like Long and Short QT syndromes etc. Cardiac arrests can also occur in congenital heart conditions like hypertrophic Obstructive Cardiomyopathies. I believe that something similar happened during the European soccer tournament to Christian Erikson of Denmark.
Can he come back and play football again? The answer is not right away. He is currently in critical but stable condition in the ICU. Looking at how quickly they got to him, it will be highly unlikely that he suffered any protracted ischemia to his brain or heart. Once he is off the ventricular, he will probably go through a boatload of testing, probably starting with brain and heart scans and testing, then a thorough cardiovascular testing which might even include genetic studies to make sure he is not harboring any inherited heart electrical channel diseases before being cut loose. If there are no contraindications or no high risk findings then he should be okay to play again, but not until he has an AICD (cardiac defibrillator) implanted.
The decision to implant a defibrillator in his chest will be made based on what his doctor's ultimately decide was the cause of his cardiac arrest. AICD's or defibrillators are often implanted when a cardiac arrest occurs spontaneously without provocation. In those circumstances we say that you suffered a primary arrest. In that case the indication for giving you the AICD is for secondary prevention of sudden cardiac death, because we fear that if you had an arrest without provocation then it can happen again, and the only sure way to save your life from another arrest, is to give you a defibrillator. That defibrillator DOES NOT DO ANYTHING TO FIX THE CAUSE OF THE PROBLEM. Its only role is to sit there and watch your heart, and if it picks up another cardiac arrest from a bad rhythm looming, then it starts to do some things to try to break the rhythm without actually shocking you. If those series of initial things fail, then it will deliver a predetermined amount of electric power to the heart to break the rhythm.
In this particular case if they decide that in fact the chest trauma caused his arrest then it will be deemed a reversible event, and he might not need an AICD, for as long as he doesn't go back to play football again because such an event can happen again as long as he is on the field tackling people head-on (or chest-on) like he did.
If on the other hand, they decide that this was some primary arrest which happen to strangely conincide with that tackling, highly unlikely though, then they will have to implant the AICD for secondary prevention as initially explained. The fact is we don't know but I trust that his doctors will do their best.
We wish him a speedy recovery.
I hope this helps to clarify for you what happened.
Disclaimer: I am NOT an electrophysiologist (EP) or a cardiac electrician. I am just a cardiac plumber 😀 so my electrician folks should feel free to clarify or add to anything I may have missed or misrepresented.
Authored by: Collins A. Kwarteng MD, FACC Founder and CEO of City of Hope Heart and Vascular Center Clinics LLC - Dublin GA, Beverly Hills CA and Las Vegas NV)
